New guidelines issued for managing peri- and postoperative atrial fibrillation
he American Association for Thoracic Surgery (AATS) has released new evidence-based guidelines for the prevention and treatment of perioperative and postoperative atrial fibrillation (POAF) and flutter for thoracic surgical procedures. The guidelines are published in The Journal of Thoracic and Cardiovascular Surgery.
“These guidelines have the potential to prevent the occurrence of atrial fibrillation in thousands of patients who undergo lung surgery in the United States each year. The AATS is committed to its goal of improving the care of patients around the globe who undergo cardiothoracic surgery each year. These guidelines will have a very positive impact on the outcomes of these patients,” commented David J. Sugarbaker, MD, Director of The Lung Institute and Professor of Surgery, Baylor College of Medicine in Houston, TX, and Past President of the AATS.
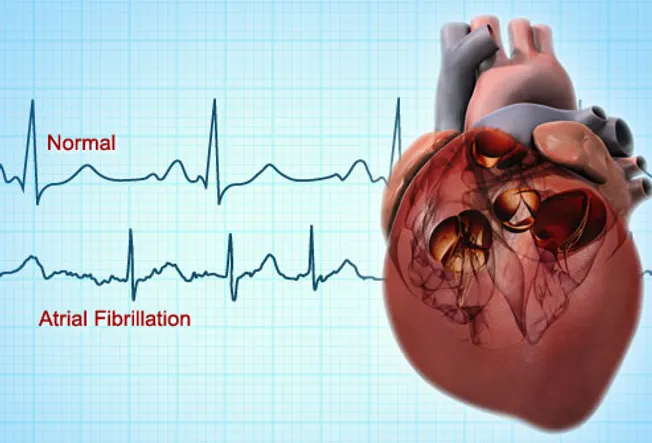
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia, occurring in one to two percent of the general population. Many studies show an increase in mortality in patients with POAF, although it is not clear to what extent the arrhythmia itself contributes to mortality. POAF is also associated with longer intensive care unit and hospital stays, increased morbidity, including strokes and new central neurologic events, as well as use of more resources. Patients who develop POAF tend to stay two to four days longer in the hospital.
A task force of sixteen experts, including cardiologists, electrophysiology specialists, anesthesiologists, intensive care specialists, thoracic and cardiac surgeons, and a clinical pharmacist, was invited by the AATS to develop evidence-based guidelines for the prevention and treatment of perioperative/postoperative atrial fibrillation and flutter (POAF) for thoracic surgical procedures.
“Patients with preexisting AF represent a high-risk population for stroke, heart failure, and other POAF-related complications,” says Gyorgy Frendl, MD, PhD, of the Department of Anesthesiology, Perioperative Critical Care and Pain Medicine, Brigham and Women’s Hospital and Harvard Medical School, Boston, MA, who co-chaired the task force. “Some may present with valvular heart disease. The management of their antiarrhythmic medications and their perioperative anticoagulation may pose a challenge.”
The task force examined evidence and adapted a standard definition for POAF. The task force also developed a set of recommendations for how to:
Define and diagnose POAF
Use physiologic (ECG) monitoring of patients at risk for POAF
Best manage and treat POAF
Use rate control and antiarrhythmic drugs, considering their mechanism of action, side effects, and limitations
Best manage the patient with preexisting AF
Manage anticoagulation for new-onset POAF
Manage (long-term) and how to follow patients with persistent new-onset POAF
 Among the task force’s main recommendations are:
Among the task force’s main recommendations are:
Both electrophysiologically-documented AF and clinically diagnosed AF should be included in the clinical documentation and reported in clinical trials/studies.
Patients at risk for POAF should be monitored with continuous ECG telemetry postoperatively for 48 to 72 hours (or less if their hospitalization is shorter) if they are undergoing procedures that pose intermediate or high risk for the development of postoperative AF or have significant additional risk factors for stroke, or if they have a history of preexisting or periodic recurrent AF before their surgery.
In patients without a history of AF, who show clinical signs of possible AF while not monitored with telemetry, ECG recordings to diagnose POAF and ongoing telemetry to monitor the period of AF should be immediately implemented.
Recent evidence suggests that some prevention strategies, such as avoiding beta-blockade withdrawal for those chronically on those medications and correction of serum magnesium when abnormal, may be effective in all patients for reducing the incidence of POAF, but that some of these strategies are underused. The task force recommends that:
Patients taking beta-blockers before thoracic surgery should continue them (even if at reduced doses) during the postoperative period to avoid beta-blockade withdrawal.
Intravenous magnesium supplementation may be considered to prevent postoperative AF when serum magnesium level is low or it is suspected that total body magnesium is depleted.
Digoxin should not be used for prophylaxis against AF.
Catheter or surgical pulmonary vein isolation (at the time of surgery) is not recommended for prevention of POAF for patients who have no previous history of AF.
Complete or partial pulmonary vein isolation at the time of (even bilateral) lung surgery should not be considered for prevention of POAF, as it is unlikely to be effective.
For those patients at increased risk for the development of POAF, preventive administration of medications (diltiazem or amiodarone) may be reasonable. However, these strategies may not be useful for all thoracic surgical patients.
Guidelines for the management of patients with preexisting AF include: criteria for obtaining cardiology consults for preoperative AF; perioperative management of anticoagulation for patients on long-term anticoagulation (warfarin or new oral anticoagulants); postoperative resumption of anticoagulation; and postoperative follow-up. Specifically, catheter or surgical ablation of AF is not recommended for management of patients with postoperative AF after thoracic surgery.
“These guidelines are best used as a guide for practice and teaching. The applicability of these recommendations to the individual patient should be evaluated on a case-by-case basis, and only applied when clinically appropriate,” comments Dr. Frendl and the task force. “In addition, these guidelines can serve as a tool for uniform practices, to guide preoperative evaluations, and form the basis of large, multicenter cohort studies for the thoracic surgical community.”
###
Matt Eaton
.(JavaScript must be enabled to view this email address)
978-299-4515
American Association for Thoracic Surgery